Runnable R recipes for clinical research: a Table 1 with gtsummary, logistic regression with odds ratios and ROC/AUC, Cox proportional hazards with assumption checks, and diagnostic test accuracy — all reproducible.
The analyses we run most often for clinical and health-sciences research, as copy-paste R you can adapt to your own data. Every table and figure below is generated live by R when this page builds — nothing is a screenshot. The examples use the built-in gtsummary::trial clinical-trial dataset and survival::lung, so they run anywhere.
The first table in almost every clinical paper: participant characteristics by group, with the right summary per variable type and a test column. gtsummary does it in a few lines.
Table 1. Baseline characteristics by treatment arm
Characteristic
Overall
N = 2001
Drug A
N = 981
Drug B
N = 1021
p-value2
Age (years)
47 (38, 57)
46 (37, 60)
48 (39, 56)
0.7
(missing)
11
7
4
Grade
0.9
I
68 (34%)
35 (36%)
33 (32%)
II
68 (34%)
32 (33%)
36 (35%)
III
64 (32%)
31 (32%)
33 (32%)
T Stage
0.9
T1
53 (27%)
28 (29%)
25 (25%)
T2
54 (27%)
25 (26%)
29 (28%)
T3
43 (22%)
22 (22%)
21 (21%)
T4
50 (25%)
23 (23%)
27 (26%)
Marker level (ng/mL)
0.64 (0.22, 1.41)
0.84 (0.23, 1.60)
0.52 (0.18, 1.21)
0.085
(missing)
10
6
4
1 Median (Q1, Q3); n (%)
2 Wilcoxon rank sum test; Pearson’s Chi-squared test
Continuous variables get median (IQR), categoricals get n (%), the test is chosen automatically, and missing data is counted explicitly rather than silently dropped.
Binary outcomes
2. Logistic regression — odds ratios & ROC/AUC
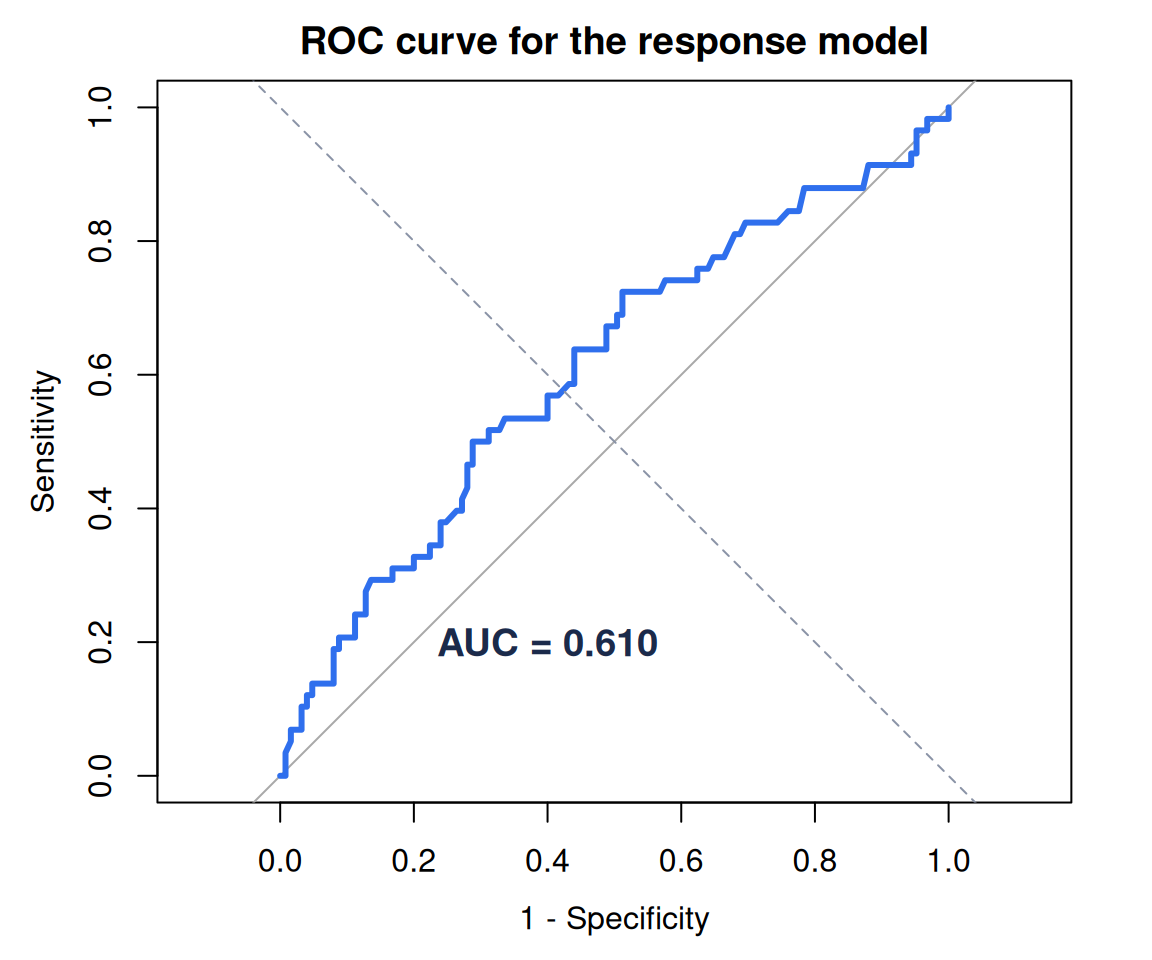
For a binary outcome (here, tumour response), fit a logistic model, report adjusted odds ratios with confidence intervals, then quantify discrimination with the ROC curve and AUC.
library(survival)d <-na.omit(trial[, c("response", "age", "grade", "stage")])fit <-glm(response ~ age + grade + stage, data = d, family = binomial)tbl_regression(fit, exponentiate =TRUE) |>bold_p() |>modify_caption("**Adjusted odds ratios for tumour response**")
Adjusted odds ratios for tumour response
Characteristic
OR
95% CI
p-value
Age
1.02
1.00, 1.04
0.092
Grade
I
—
—
II
0.84
0.38, 1.85
0.7
III
1.05
0.49, 2.25
>0.9
T Stage
T1
—
—
T2
0.57
0.23, 1.34
0.2
T3
0.91
0.37, 2.22
0.8
T4
0.76
0.31, 1.85
0.6
Abbreviations: CI = Confidence Interval, OR = Odds Ratio
library(pROC)roc_obj <-roc(d$response, fitted(fit), quiet =TRUE)plot(roc_obj, col ="#2f6fed", lwd =3, legacy.axes =TRUE,xlab ="1 - Specificity", ylab ="Sensitivity",main ="ROC curve for the response model")abline(0, 1, lty =2, col ="#8a93a6")text(0.6, 0.2, sprintf("AUC = %.3f", as.numeric(auc(roc_obj))),col ="#1b2a4a", font =2, cex =1.2)
Figure 1
The odds-ratio table answers “which factors matter, and by how much?”; the AUC answers “how well does the model separate responders from non-responders?”
Time-to-event
3. Cox proportional hazards — with assumption checks
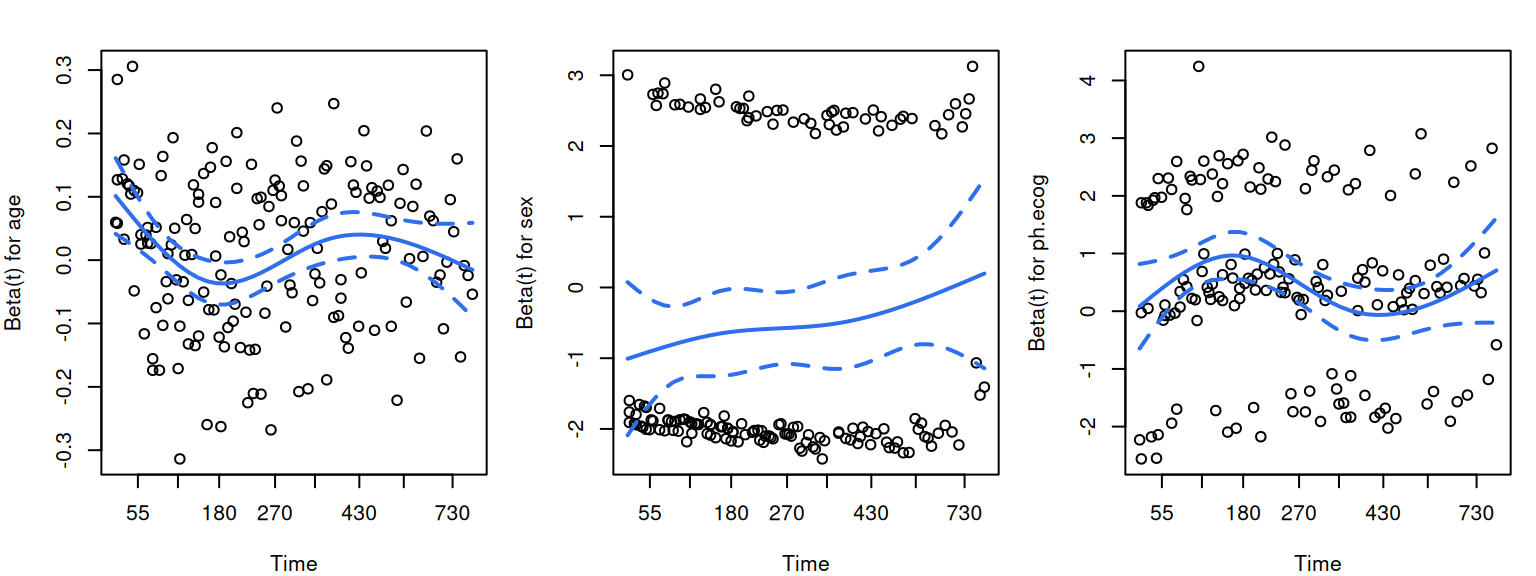
A hazard ratio is only trustworthy if the proportional-hazards assumption holds. Fit the model, report hazard ratios, then test the assumption with cox.zph() — never skip the second step.
cx <-coxph(Surv(time, status) ~ age + sex + ph.ecog, data = lung)tbl_regression(cx, exponentiate =TRUE,label =list(sex ~"Sex (2 = female)", ph.ecog ~"ECOG performance score")) |>bold_p() |>modify_caption("**Hazard ratios, advanced lung cancer (survival::lung)**")
Hazard ratios, advanced lung cancer (survival::lung)
Characteristic
HR
95% CI
p-value
age
1.01
0.99, 1.03
0.2
Sex (2 = female)
0.58
0.41, 0.80
<0.001
ECOG performance score
1.59
1.27, 1.99
<0.001
Abbreviations: CI = Confidence Interval, HR = Hazard Ratio
zph <-cox.zph(cx)zph
chisq df p
age 0.188 1 0.66
sex 2.305 1 0.13
ph.ecog 2.054 1 0.15
GLOBAL 4.464 3 0.22
par(mfrow =c(1, 3), mar =c(4, 4, 2, 1), family ="sans")plot(zph, col ="#2f6fed", lwd =2)
Figure 2
A non-significant global test (and flat scaled-Schoenfeld residuals) means proportional hazards is a defensible assumption. A small p is a warning, not a verdict — it points you toward stratification, time-varying effects or a different model.
Screening & tests
4. Diagnostic test accuracy
Sensitivity, specificity, predictive values and likelihood ratios from a 2×2 table — the numbers a clinician actually asks for. Base R, no dependencies.
Remember that predictive values depend on prevalence — the same test looks very different in a screening population versus a specialist clinic. When that matters, we model PPV/NPV across the plausible prevalence range (try the diagnostic-test calculator in our live demos).